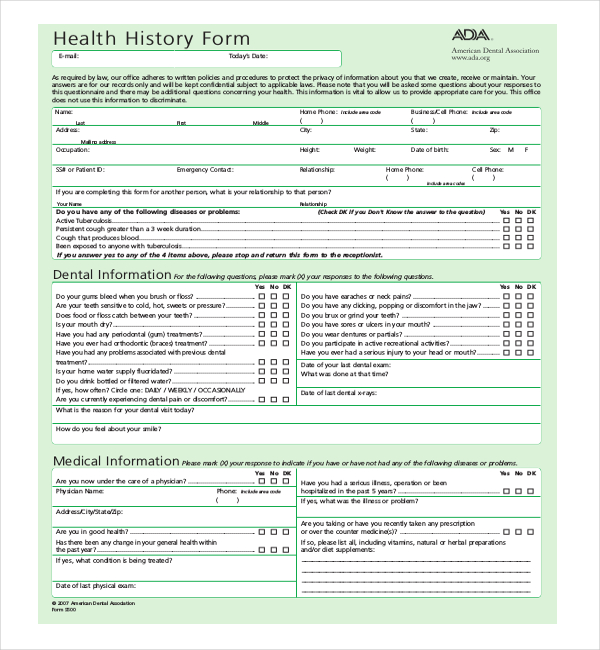
Use this health history form questionnaire to collect the data you need before a patient's first appointment to reduce waiting room delays. Labbe's personal calendar to book your free Clarity Call at a time that works for you. Health ( e-mail: history form today's date: a d)a. american dental association.ada.org as required by law, our office adheres to written policies and procedures to protect the privacy of information about. Please note that your session will automatically end after.

Health ( e-mail: history form today's date: a d)a. american dental association.ada.org as required by law, our office adheres to written policies and procedures to protect the privacy of information about.
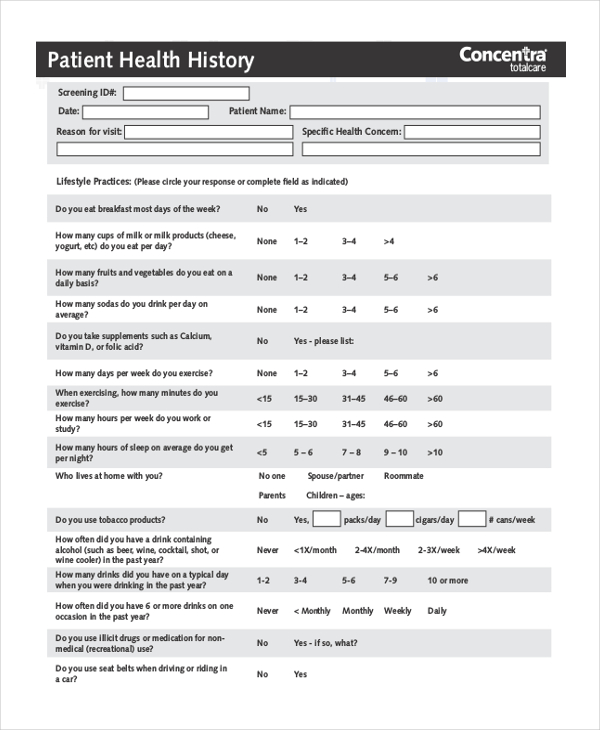
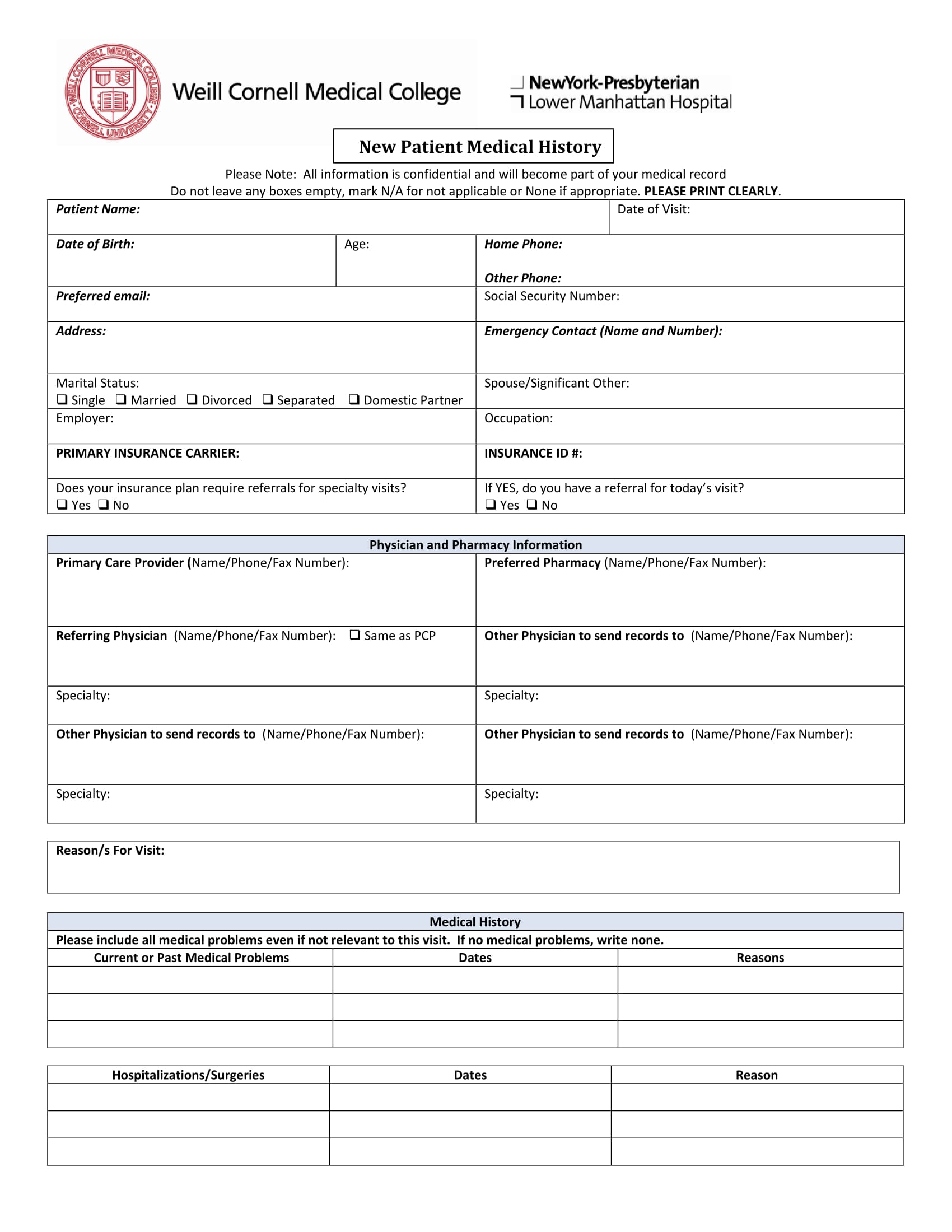
The patient health history form can have other names like medical history form or family health history form. Here is a preview of the patient health history questionnaire forms. Use this health history form questionnaire to collect the data you need before a patient's first appointment to reduce waiting room delays.
Can you fax a new copy to me?

Health ( e-mail: history form today's date: a d)a. american dental association.ada.org as required by law, our office adheres to written policies and procedures to protect the privacy of information about.
In this video, we will show you how to upload your Health History Form in myhealth.uconn.edu.
Health ( e-mail: history form today's date: a d)a. american dental association.ada.org as required by law, our office adheres to written policies and procedures to protect the privacy of information about.
Use this health history form questionnaire to collect the data you need before a patient's first appointment to reduce waiting room delays.
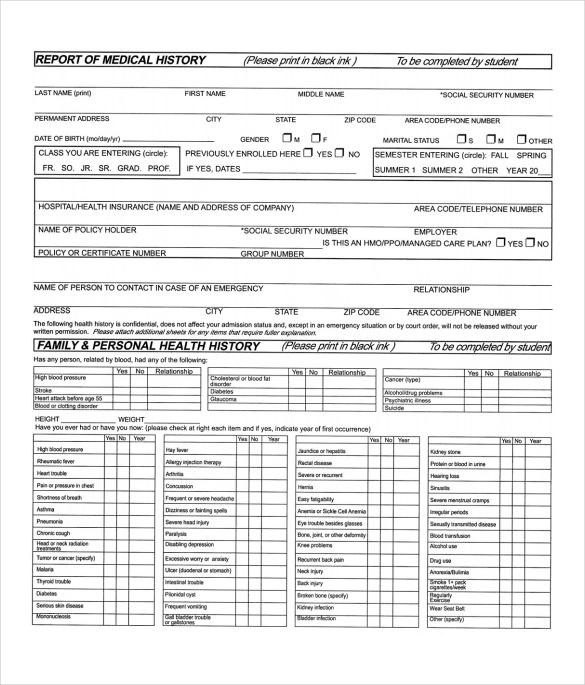
You will NOT be eligible to register for classes until this form has been completed in full and reviewed by the health center staff.
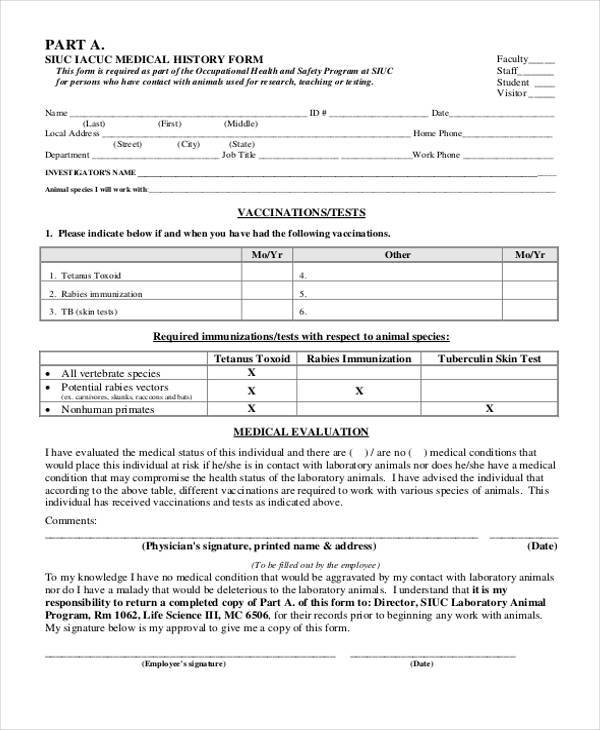
After the health history, baseline measurements, and vital signs are done, you should do all but which of the following? Can you fax a new copy to me? The form template covers personal health history, health habits and personal safety. The patient health history form can have other names like medical history form or family health history form. HEALTH HISTORY FORM Form must be filled out and submitted with Immunization Form MENTAL HEALTH HISTORY: Have you ever suffered from/been treated for/been hospitalized for the following?

In this video, we will show you how to upload your Health History Form in myhealth.uconn.edu.
In this video, we will show you how to upload your Health History Form in myhealth.uconn.edu.
![67 Medical History Forms [Word, PDF] - Printable Templates](https://printabletemplates.com/wp-content/uploads/templates/medical-history-form/medical%20history%20form%2013-768x994.jpg)
Childhood illness By signing this form, you consent to our use and disclosure of protected health information about you for treatment, payment and health care.
Can you fax a new copy to me?
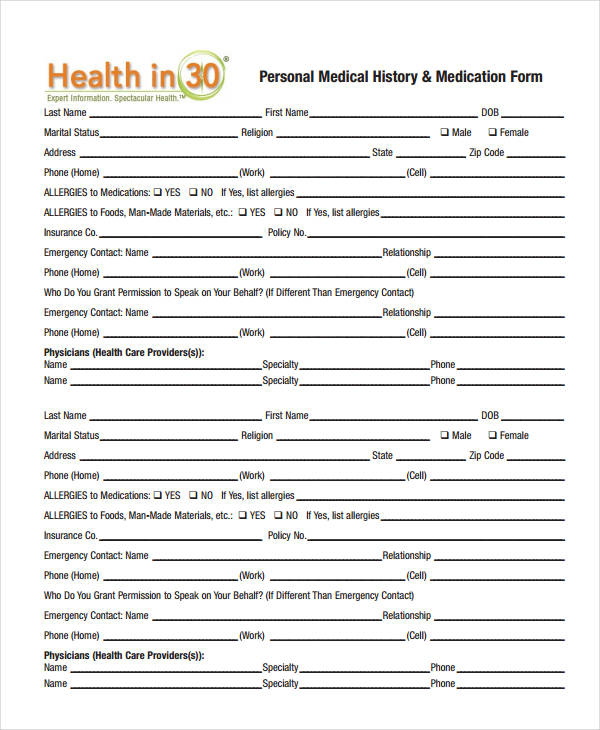
Review the information, then click the Health History Form for New Students link at the bottom of You will now be in the Health History Form. Health Insurance information University Wellness Services has the capability to bill your insurance company for the services provided. Give your patients the freedom to complete medical The purpose of the medical history form is to show the physician important information regarding the. Health ( e-mail: history form today's date: a d)a. american dental association.ada.org as required by law, our office adheres to written policies and procedures to protect the privacy of information about.